No, not as in physically trying to reach my foot – I can still do that … just about! This was about trying to get the therapy to reach my foot.
All change at Medtronic … again
Yesterday I had another appointment with Mr Mundil and the Medtronic tech to look at the programming of my device. The primary aim was to see if the existing device could be programmed to target the neuropathy in my foot. This has become increasingly problematic over the last few months, particularly whenever my leg is elevated. Consequently sleeping is an issue, or more specifically getting to sleep. I did add though that, following a discussion with the clinical pharmacist at the GP practice, I am now taking 200mg Pregabalin in the evening, and that seems to be helping with my foot, whilst not causing brain-fog the following day. It does take me a little longer to get going in the mornings though. But then again, maybe that is just down to dampened enthusiasm due to the dark (and mostly wet) mornings and the fact I am faced with yet another morning of having to drag a dog out who regularly shows his complete disinterest in going out for a walk. I’m sure he thinks he is reluctantly taking me out for my benefit rather than the other way around! 🤷♂️
Following Sam’s departure from Medtronic earlier in the year, as we were making our way from the waiting area to the clinic room Mr Mundil explained that Nima has now also left Medtronic, and so Chris has taken over the role. Mr Mundil was encouraging about his experiences with Chris so far.
Deal with the new back pain first
I explained that, for a few weeks now I have had more back pain in slightly different areas to where it normally spikes. It has been both directly to the left of the right shoulder-blade, pretty much on the spine itself, and also directly below the right shoulder-blade, perhaps 7 or 8cm down. We therefore started with seeing if the existing therapy could be spread a bit wider to cover these areas. First off Chris checked the impedances of the paddle electrode and everything was working fine. He was extremely thorough, trying all sorts of settings to try to get the best coverage, and then fine-tune the ECAPs function so that the closed-loop function triggered at the right point when I get a spike in pain/overstimulation. Ultimately he concluded the existing programs – one for day and one for night – were correct, but he would broaden the pulse width to improve coverage. All seemed sensible.
Now then, about that foot
I was already aware from previous discussions, but Mr Mundil reiterated that, because the paddle electrode is so high in my neck, it was a bit of a long shot to be able to target my foot, and even if it was possible it might cause issues elsewhere. It would also have to be a completely separate program, so I would have to select to use it when my foot is bad, and therefore stop the therapy for by back. Chris started with the new programme. He explained that he would start it on a very low strength so I didn’t get a sudden shock. Whilst Mr Mundil and I were chatting about other things, Chris was sat next to me gradually increasing the strength and constantly checking with me where I could feel any tingling. The answer each time was no. This went on for several minutes, and I could hear the clicks as Chris upped the level by greater steps each time, but still nothing. I did at one point think I felt a slight twinge across the top of my foot, but as Chris increased it even further without any other signs, I concluded that twinge was just my usual foot doing odd things. Eventually Mr Mundil said he felt we should accept it won’t work. Given the complete lack of anything happening, I had to agree. Whilst he didn’t actually say it, the look on Chris’s face suggested he was surprised at how strong a signal he was trying to use.
Oh well, we knew it was a long-shot, but it was worth a go.
So where-to next?
Whilst Chris was trying to target my foot, Mr Mundil was updating me on other discussions he’d been having about how to deal with my foot whilst maintaining the therapy for my back. We had briefly spoken before about a second stimulator. It would appear this is not always successful, with quite a lot of patients reporting they lose some, and occasionally a lot of the benefit of the original device when the second is fitted. He also feels that, because I am still mobile to an extent (I’m not in a chair permanently), he would need to fit another paddle electrode, rather than a wire. Thus the procedure would be extremely invasive – like the previous stims. A daunting prospect of going through that for a third time. Well 5th time if you include the two attempts to correct my spinal cord back in 2016 and 2017.
The other thing Mr Mundil gave me an update on was the potential availability of Qutenza at the hospital. It is looking more promising that the pain service will be able to start this treatment, albeit probably not until the summer of 2026. By the time we’d finished chatting about this, we’d reached the point where he felt there was no point continuing trying to target my foot. I said that, whilst I’m not exactly enthralled about the idea of going through significant invasive surgery again, particularly with the outcomes others have experienced having two stims, I’m not ready to rule that out. However, the focus for now will be continuing to track the development of the Qutenza service at the hospital, and see if/how that benefits me when I can get started. In the meantime, I will continue with the new programmes for my back, stick with the increased dose of pregabalin at night, and use lidocaine patches on my foot.
But wait. This is not what I expected!
Ok, so the above is the situation had I written this after the appointment as I had intended. But I didn’t, I’m writing it the next day having discovered something and had night to (not) sleep on it. 🥱
When I opened the MyStim app on the remote to change to the night programme late yesterday evening I discovered that, not only did I have the old (non-closed-loop) programme (Group C) and the two I’ve been using (group D for evening and group E for day – don’t ask why that way round! 🤦♂️) adjusted for the broadened pulse width, I also have groups F and G.
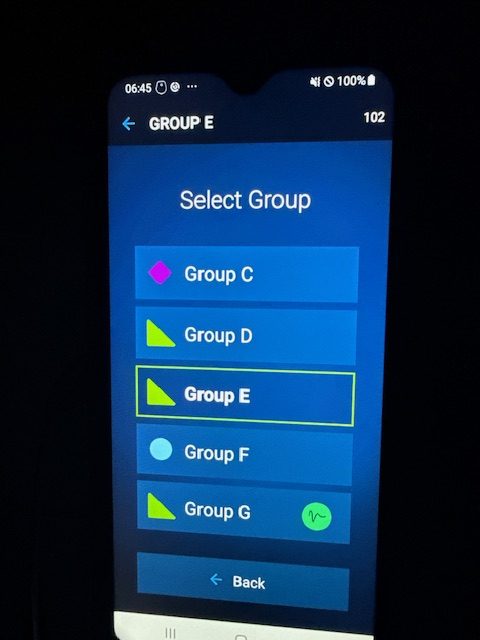
My understanding was that Chris had tweaked D and E, rather than adding new programmes. If he has added the tweaked ones as new programmes, then why do they have different symbols, as this suggests they are different types of programme rather than tweaks to copies of the originals. Nima had explained that the icon next to group C denotes it is a standard programme, whereas the green triangle denotes an ECAPS (closed loop) programme. What do the blue circle on group F and the waveform on group G mean? Why are they just not the same as for D and E, which they should be replacing?
Initially I changed to D, my usual night programme, but I got instant overstimulation at even moderate neck movement. If it was like that sitting on the sofa, by the time I laid in bed that would be amplified. I then thought, well if Chris added F and G as replacements for D and E, then maybe F is the right one for night. F was less intense, and the overstimulation was all in the left arm, whereas I can’t usually feel anything on the left if I have therapy on the right (something that baffled the Abbott tech when I had their device). I tried G and when I tipped my head slightly forward to look at the screen again, I nearly shot out the chair the overstim was so great. I put it back onto E and finished what I needed to do before going to bed.
Once in bed I went through them again incase any were actually better when I was lying down. They weren’t! As I pretty much expected, any level of overstimulation I had sat down was increased when I laid down. I was hoping D would at least be the same as I’d had prior to the reprogramming (on the basis perhaps Chris had left D and E alone and added the new tweaked copies. The only one I could be moderately comfortable with was my day programme – E. Even with that though I was susceptible to overstimulation when I moved in bed (the main reason D was created for night as the tolerance before ECAPS does it’s thing were adjusted). So what with that, and the fact my foot was deciding to have one of its bad nights, sleep was very intermittent.
The lack of sleep did mean that, not only was I able to finish the Guardian’s killer sudoku, but I was also able to email the neurosurgery team with what has been happening, and do some extensive research into what the various symbols on the MyStim app mean. When I say I did some extensive research, what I mean is that I got ChatGPT to do some extensive research. It trawled the Medtronic Inceptive manuals and found some useful stuff. You can read the full response here, but in specific relation to the symbols agains my programmes they can be summarised as:
| Icon | Meaning |
|---|---|
| Pink diamond | Standard fixed stimulation |
| Green triangle | Closed-loop (NeuroSense) automatic ECAP-based adjustment |
| Blue circle | AdaptiveStim posture-responsive therapy |
| Green circle with waveform | Special waveform mode (often paired with closed-loop) |
Call-back from neuro team
Mid-morning I had a call back from Lincey, one of the specialist nurses in the neuro team. She had spoken to Chris regarding my email. He doesn’t believe he touched programmes D and E, so is surprised I am getting different sensations. Lincey has given him my number and I can expect a call back. Unfortunately, unlike the Abbott Proclaim device I had previously, they cannot programme it remotely, so I will have to go back in at some point to have any changes made. In the meantime it is a case of making the best I can of the programmes I’ve got.